9th February 2026 9:00 am
- 10th February 2026 12:00 am
- 10th February 2026 12:00 am
International Osteosynthesis Course – Osteosynthesis on the human specimen
ITS. Headquarters Autal 28, 8301 Lassnitzhöhe
Established in October 2013, LEDA Orthopaedics began life as a sales agency and quickly grew into a leading orthopaedic distributor in the UK and Europe, working with innovative suppliers from all over the world. Founding directors David Plane and Jon Bloy have over 40 years’ collective experience in the orthopaedic industry and a passion for the sector that shines through in their ongoing commitment to the business to this day. Read More…
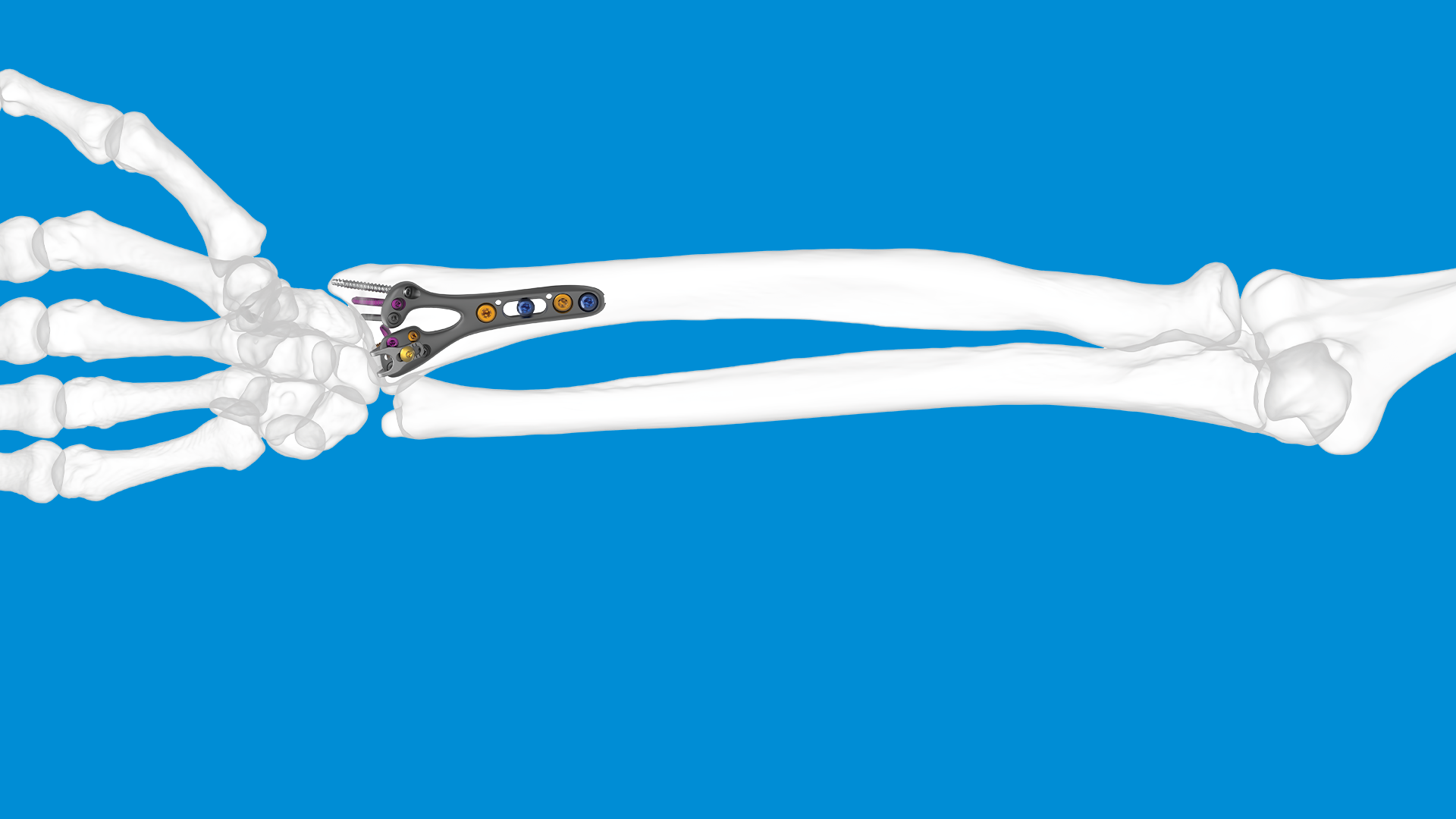










The carpometacarpal (CMC) joint of the thumb (also called the trapeziometacarpal joint) is highly mobile and is subjected to considerable forces during pinch, grip, and dexterous tasks. This combination makes it vulnerable to degenerative changes, overuse, trauma, and instability. When conservative measures fail to deliver adequate pain relief or function, surgical intervention becomes a consideration.
Understanding when surgery is appropriate, which surgical options exist, and what outcomes to expect is essential for both patients and clinicians. In the UK, the British Society for Surgery of the Hand (BSSH) has produced the BEST guideline on thumb base osteoarthritis, which provides structured recommendations.
Below, we review:
The thumb CMC joint sits between the base of the first metacarpal and the trapezium bone of the wrist. It allows flexion/extension, abduction/adduction, and a degree of axial rotation (opposition). Over time, or after trauma, cartilage degeneration, subchondral sclerosis, osteophyte formation, and joint subluxation may develop, leading to osteoarthritis.
Because the joint must both bear load and allow mobility, degeneration frequently ends up producing pain, instability, and functional limitation. In more advanced cases, the joint’s alignment may shift, and secondary changes (e.g., in adjacent joints) may occur.
Typical symptoms include:
On examination, doctors often test for pain with load across the joint, “grind test” (axial compression + rotation), and assess stability. Plain radiographs are standard (AP, lateral, oblique views) to grade the severity of arthritic change, subluxation, and joint space narrowing.
Where there is ambiguity about the involvement of adjacent joints (e.g. the scaphotrapeziotrapezoidal joint, STT), further imaging may be necessary.
All patients should undergo non‑surgical management first, unless the condition is extreme.
According to the BSSH BEST guideline, a stepwise multimodal approach is recommended. Common measures include:
According to the BSSH BEST guidance, if symptoms persist despite “a comprehensive non-invasive management package” (splinting, therapy, analgesics), then surgical options can be considered.
However, it is important to emphasise that conservative measures may not completely remove all symptoms but aim to improve pain control, maintain function, and delay or avoid surgery.
Moving to surgery is a significant decision. Not every patient with thumb CMC osteoarthritis is a surgical candidate, and not all surgical techniques are appropriate for everyone. The decision should balance symptom severity, functional limitation, patient expectations, comorbidities, and risk vs benefit.
Here are key indications, contraindications, and decision factors:
The BSSH BEST guideline suggests that if symptoms fail to resolve after non-invasive management, surgery should be considered.
Once surgery is judged to be the right option, surgeons may choose among several techniques. The most common ones include:
Each has advantages, drawbacks, and evidence.
This is the “classic” and still most commonly used operation. It involves removing the trapezium bone to eliminate the arthritic articulation. Some surgeons may leave the gap (simple resection), while others may stabilise the thumb metacarpal using soft tissue interposition or tendon grafts.
Pros:
Cons:
The BSSH BEST guideline notes that additional procedures (interposition or ligament reconstruction) do not appear to confer major benefit over simple excision (trapeziectomy alone) in their systematic evaluation.
To address concerns about instability or metacarpal collapse, surgeons often pair trapeziectomy with a soft tissue procedure — e.g. using a strip of the flexor carpi radialis (FCR) tendon to reconstruct ligaments or interpose tissue in the gap (thus stabilising the thumb).
Pros:
Cons:
Fusion of the CMC joint is less common and is typically reserved for younger patients or in specific circumstances. By fusing the joint, pain is eliminated but mobility is sacrificed.
Pros:
Cons:
Because of the mobility lost, fusion is used selectively (e.g. high demand or where implant options are not favourable).
This involves replacing the articulating surfaces with a prosthesis (either full or partial). Several designs exist: total CMC implants, hemiarthroplasty, or synthetic cartilage implants (e.g. the MAIA implant) in more recent practice.
Pros:
Cons:
The MAIA implant could be an excellent option given its claimed advantages:
To find out more about MAIA, please visit our dedicated page: MAIA – CMCJ Replacement – LEDA.
One clinical series of cemented total trapeziometacarpal implants in advanced disease (Eaton stage III/IV) showed good outcomes at average 59 months: most patients were pain-free; average pinch strength ~85% of the unaffected side; minimal loosening in follow-up.
In the UK, when using implants like MAIA, aftercare protocols typically involve cast / splint immobilisation initially, followed by rehabilitation over weeks to months.
Trapeziectomy remains a gold standard in many UK services, partly because of its reliability and lower risk of long-term implant complications; the BEST guideline acknowledges prosthetic techniques but highlights the need for balanced decision-making.
Common risks to discuss include:
To help patients decide, the clinician should:
Here is a simplified decision pathway:
The BSSH BEST guideline endorses a stepwise approach, whereby surgery is reserved for those who do not respond to conservative treatment.
To explore differences in stability between a trapeziometacarpal prosthesis and trapeziectomy/ligamentoplasty, please see the clinical paper linked below:
Hyperextension MP.pdf
In today’s dynamic orthopaedic and trauma device marketplace, choosing the right distribution or commercial partner is a strategic decision. LEDA Orthopaedics has built a reputation as a responsive, clinically engaged, and quality‑driven UK orthopaedic distributor. For implant and device manufacturers, hospitals, clinical services, and surgical teams, partnering with LEDA can bring distinct advantages. Here are five compelling reasons to consider:
One of our differentiators is our emphasis on procedural knowledge, clinician engagement, and personalised advisory support rather than just transactional supply. LEDA is not a passive distributor: we aim to provide “consultative procedural knowledge and personal product advice” to our clientele.
In the orthopaedic field, where device selection, surgical technique, and intraoperative decision-making are interdependent, this consultative posture helps mitigate risk, improves adoption success, and builds trust with surgeon users. Many manufacturers struggle when distributors lack clinical depth; LEDA’s model helps bridge that gap.
LEDA operates as an independent, UK-based specialist orthopaedic distributor, established in 2013, with a focus on upper-limb, foot & ankle, trauma, and niche orthopaedics.
This relatively lean, focused approach confers several advantages:
Large distributors often have rigid systems, lengthy lead times, or diluted attention to smaller product lines. A specialist partner like LEDA can nurture emerging technologies and give them the attention they deserve.
Partnering with LEDA provides access to a curated portfolio of orthopaedic and trauma technologies, some of which we hold exclusive distribution rights in the UK & Ireland:
For a device manufacturer, this breadth means less fragmentation of sales channels and consistency in representation across hospital specialties. For clinical customers, it means more synergy and convenience from having a trusted vendor across multiple product lines.
Any credible partner in the UK orthopaedics space must align with standards of quality, transparency, and ethics. Our public profile and activities suggest we take this alignment seriously:
For manufacturers and clinicians, partnering with an entity that understands and respects the demands of audit, regulatory compliance, and conflict-of-interest transparency is a strong safeguard.
We are not just a distributor; we position ourselves as partners in innovation and growth.
For example:
If a manufacturer or innovator wants a UK foothold, LEDA can act as a conduit for clinical trials, key opinion leader relationships, registry data collection, and surgeon engagement.
To illustrate the synergy, here’s how a hypothetical collaboration might look:
Over time, this approach helps build trust, drive adoption, reduce friction in procurement and clinical integration, and ultimately improve patient outcomes.
In summary, here are the five key reasons to partner with LEDA Ortho:
If your organisation is evaluating UK distribution partners, or you are seeking a more clinically engaged, responsive, and quality-aligned collaborator, LEDA Ortho presents a compelling option. Please contact us for more information, call +44 (0) 1480 457222 or email sales@ledaortho.com.
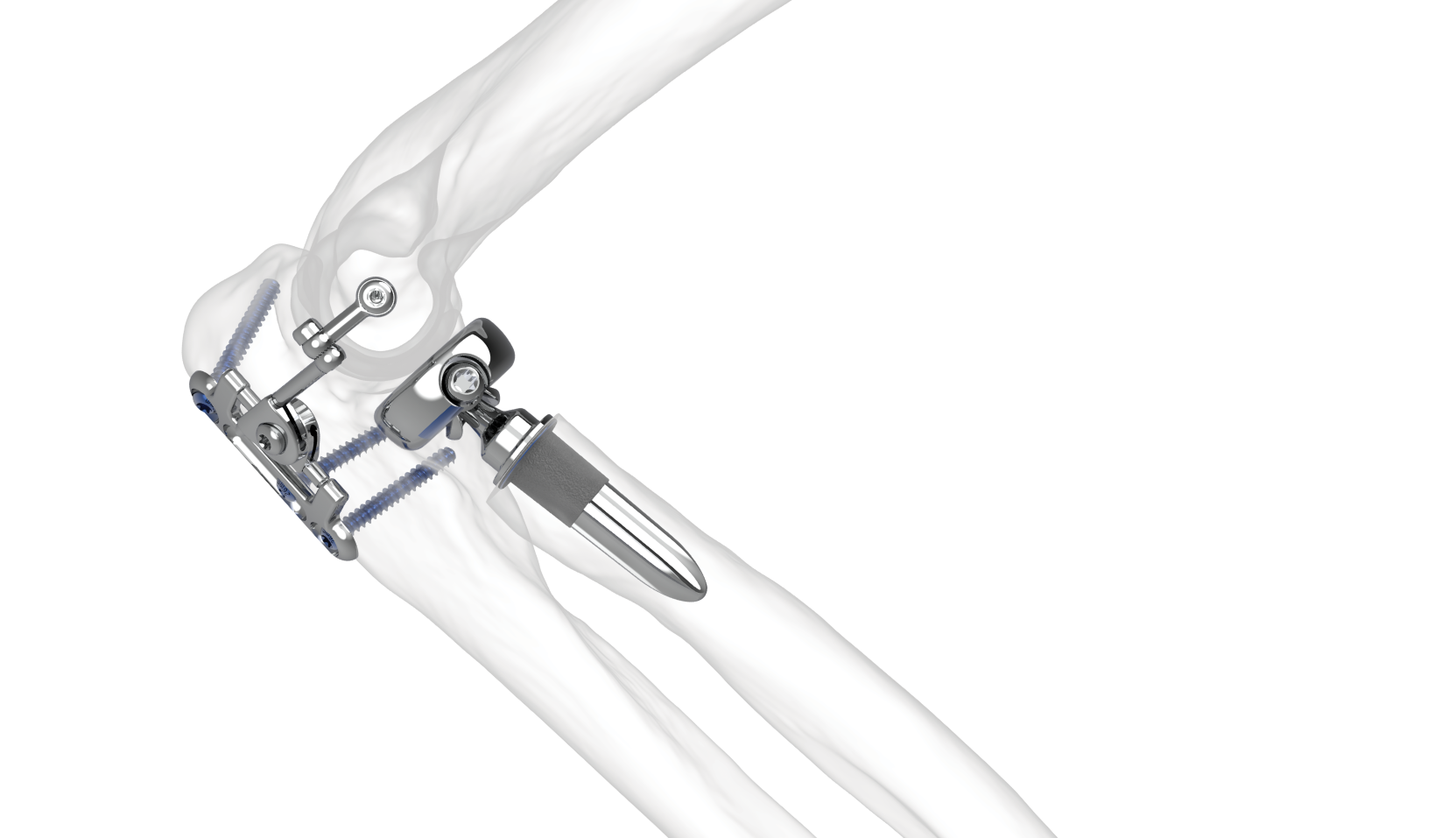
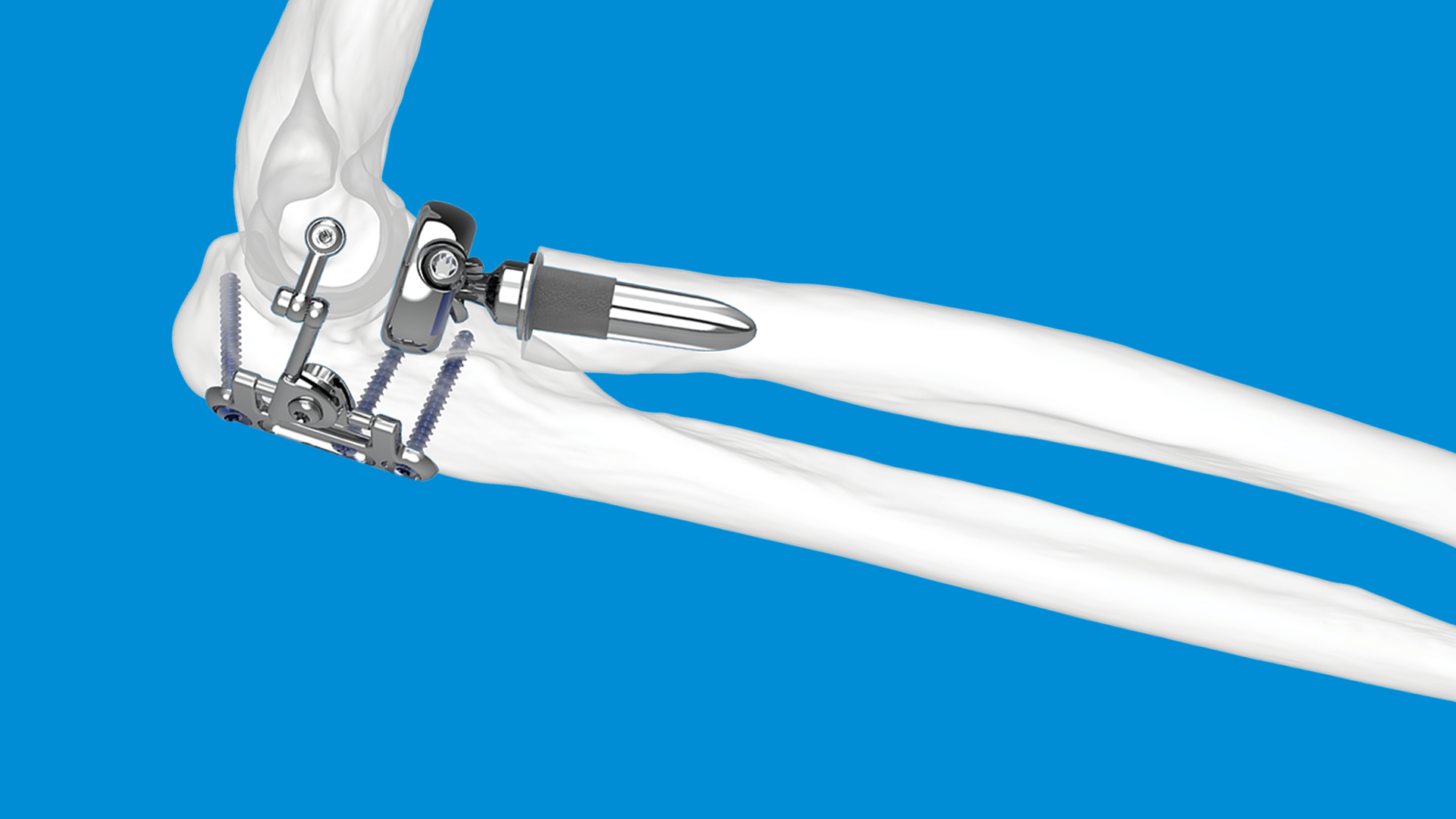
The radial head is a critical component of elbow anatomy contributing to stability, load transmission, and forearm rotation. In complex elbow injuries — such as comminuted radial head fractures, fracture‑dislocations of the elbow (e.g. “terrible triad” injuries), or associated ligamentous damage — the normal anatomy and biomechanical stability are disrupted. In such settings, radial head replacement (sometimes called radial head arthroplasty, RHA, or prosthetic replacement) has emerged as a key surgical option alongside other strategies like open reduction internal fixation (ORIF), resection, ligament repair, or combinations thereof.
To appreciate when and why radial head replacement is used, it’s useful to recall what role the radial head plays:
The Mason classification (modified) is often used to classify radial head fractures. Mason type III (comminuted fractures) or type IV (fractures with dislocation) are more severe and frequently where replacement becomes a serious option.
From the literature, the main indications are:
Using radial head replacement successfully involves careful attention to multiple surgical and implant‑based details:
Here are some key findings from recent studies:
While RHA offers many advantages, several important limitations, risks, and trade‑offs must be discussed with patients.
In the UK, specific BOA guidelines on radial head replacement are not, at least publicly, as detailed as for some other orthopaedic problems. Still:
Thus, while BOA doesn’t yet have a “definitive guideline” specifically naming every indication of radial head replacement, UK practice tends to follow the international evidence and these intra‑UK sources.
Putting together where the evidence supports it, the decision to use radial head replacement in complex elbow injury might follow roughly this pattern:
| Factor | Favors ORIF / Reconstruction | Favors Radial Head Replacement |
| Fracture pattern | ≤ 2 fragments, good articular surface, bone stock good | >3 fragments, comminution, missing articular surface, poor bone quality |
| Associated injuries | Minimal, stable elbow; ligament injury well preserved | Coronoid fracture, dislocation, LCL (+/‑ MCL) injury, elbow unstable |
| Soft tissue status & timing | Early, minimal soft‑tissue damage; early surgery possible | Delayed presentation; risk of stiffness; high‑energy injury; swelling |
| Patient factors | Young, high demand, expectations of long life in prosthesis | Older, lower demand; but needs vs risk of reoperation must be balanced |
| Surgeon & implant factors | Surgeon’s experience in ORIF; access to implants; expected outcomes | Implant type available; ability to restore size/height; repair ligaments appropriately; rehab resources |
Putting it all together, radial head replacement plays a central role in many complex elbow injuries. Key take‑home points:
There remain gaps in the evidence, which mean that practice is still evolving:
From this review, some suggested practice recommendations (based on the best available evidence) include:
Radial head replacement has become a mainstay in the management of complex elbow injuries — especially for severely comminuted fractures and associated instability (e.g. terrible triad). The evidence (albeit not always from large RCTs) suggests that when used appropriately, it restores stability, yields good functional outcomes, and offers better performance than fixation or excision alone in many settings. However, it is not a panacea: surgical technique, implant choice, patient selection, timing, and managing associated injuries all highly influence outcomes.
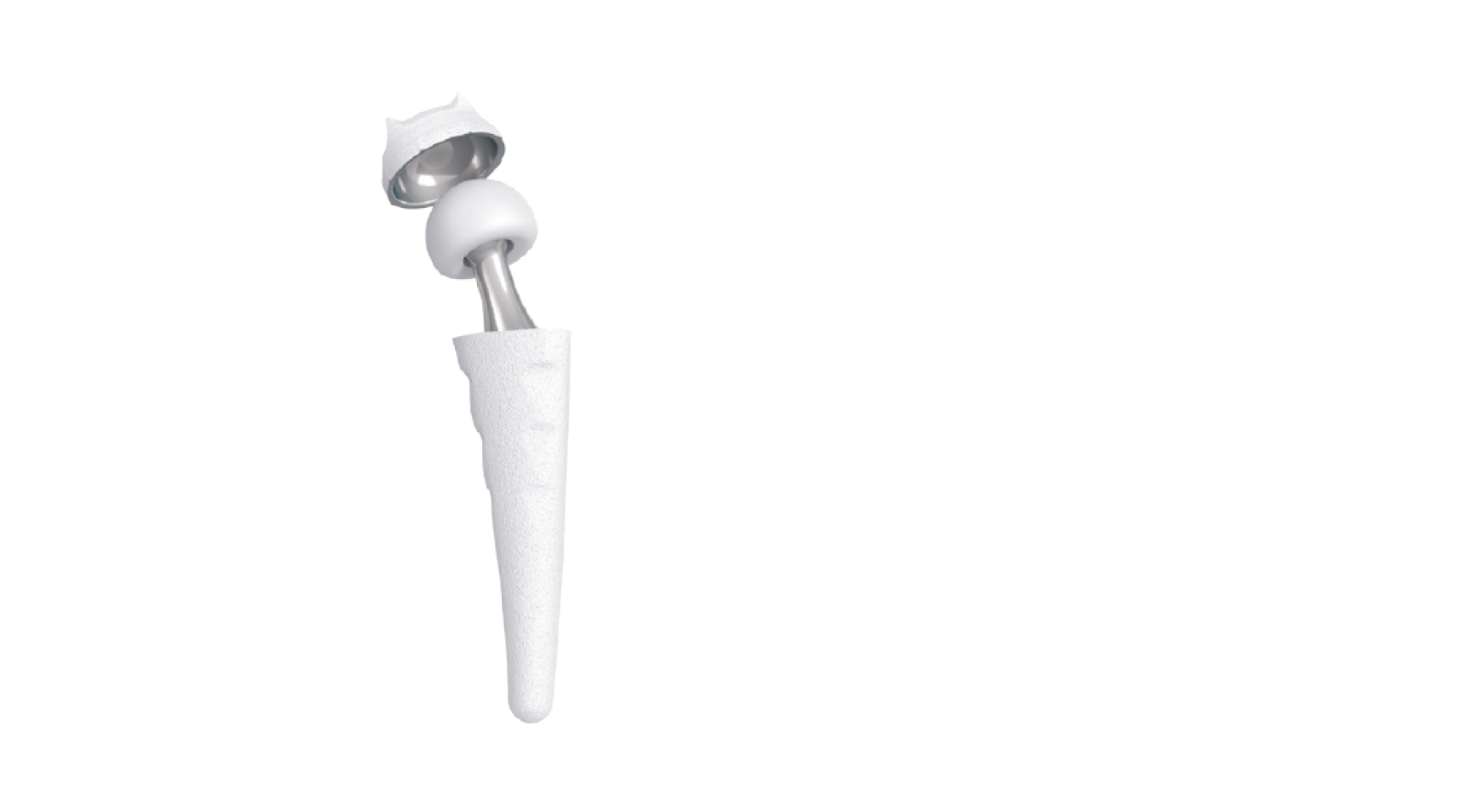
In this context, the Skeletal Dynamics ALIGN Radial Head System offers a modern, anatomically driven solution designed to support more predictable and stable outcomes. Its features reflect current thinking in elbow biomechanics and prosthetic design, including:
Together, these design elements aim to replicate native kinematics while offering the durability and stability required in complex elbow reconstructions.
If you think a radial head replacement might be indicated in your case, you may wish to explore ALIGN via our website ALIGN – Radial Head Replacement – LEDA
Take a moment to read this study on how the Skeletal Dynamics MAIA prosthesis, designed to align with the forearm’s axis of rotation, may improve patient outcomes: A radial head prosthesis that aligns with the forearm axis of rotation: a retrospective multicenter study
